
Families speak out about the urgent need to tackle sleep issues for loved ones with Down syndrome
The DSSRN exists to bring researchers together. However, the heart of this network is not just centred on advancing scientific knowledge. The network is responding to a need that is persistent and urgent, and yet seldom noticed outside caregiving circles.
We asked some family members and carers to tell us why the issue matters. In this blog, we share some of the things that family members have said, concerning ways that poor sleep acutely impacts loved ones with DS and their families.
“The negative consequences of H’s sleep deprivation are significant and far reaching. Sometimes just getting through the next day after a disturbed night is all we can manage. Sleep deprivation causes all of these things:
- Worsens her cognitive functioning and learning delays
- Contributes to her poor immune function - as a consequence she picks up more illness and infections
- Causes absences - more days are missed from school due to poor health/lack of sleep
- She rarely achieves fully restorative sleep due to constant restlessness during sleep
- Increases her sensory seeking behaviours and hyperactivity
- Heightens stress and has cumulative effects on her mental health
- Causes stress to us as her parents/caregivers, and has a knock on effect to our health and wellbeing
- Directly affects my own management of Type 1 Diabetes, and has contributed to serious illness and hospitalisation for diabetic complications brought on by stress both physical and mental
- Affects our ability to effectively carry out daily functions, such as work, managing the home, and meeting the needs of other family members
- Increased tiredness leads to mistakes being made at any level: eg, admin, driving, becoming more accident prone in the home, etc
- Makes us less likely to plan outings or activities that we might otherwise want to do, as lack of sleep takes away motivation and physical strength
- Affects our marriage and family life, and destroys being able to spend quality time together when we are always so tired
- Causes stress and anxiety as we search for ways to alleviate the problem
- Very costly due to purchasing items that may or may not help, eg, weighted blankets, compression sheets etc
- Leads to more hospital appointments and intrusive investigations such as sleep studies, which in themselves mean that we get no sleep whilst monitoring her
- Leads to hospital admissions for surgeries/procedures under General Anaesthetic eg Tonsils/Adenoids removal but with little to no improvement seen.
It feels like we go round in circles, and medics never fully understand what’s going on, or are prepared to think outside the box of the usual ‘go to’ solutions. So sleep studies get repeated, but nothing really changes.
Families like ours are routinely told to expect sleep problems as a part of having Down’s syndrome. This is simply unacceptable. This approach would not be tolerated if it was applied to the general population, who would rightly demand and expect research to look for solutions. Yet people with DS and their families are given so little hope of improvement when it comes to the significant sleep problems they experience. A sleep research network would give them hope that their difficulties may in time be overcome and their quality of life much improved.”
- AM, Parent in the DS Community
“Talk about quality of sleep is a major concern for people all over the country. Many people don’t even realise that their kids with Down syndrome probably need a sleep study, or what a bad sleep consequently means for our kids. We need multi-site studies to enable clinical trials and to develop solutions for this community.
Following a sleep study, our daughter was diagnosed with sleep apnoea. Since she started using an APAP (automatic positive airway pressure) machine, the difference has been notable. Her voice is stronger, and she no longer falls asleep so readily in the car. When she has a cold, the machine can also help ease her symptoms and support her recovery. Beyond the improvements we can see, we know it is likely benefiting her long-term health too.”
- LM, Parent in the DS Community
“Poor sleep quality means that my brother, who has Down syndrome, needs to go to bed as early as 7:30pm to get enough hours of sleep in, to allow him to function at his best during the day. As a young adult, this means he misses out on social time with his peers and can contribute to him being treated by others as a child, rather than as the young person he is. It also means he goes to bed at the same time as very young family members and that, in turn, makes him feel infantilised and affects his self-esteem.
Disturbed sleep has meant our family hasn’t taken a holiday in years because it’s too stressful to manage further disturbances caused by a change in environment. That has led, historically, to early abandon of holidays due to extreme exhaustion for everyone, and incurred financial loss therefore as well.
Sleep challenges are major, unseen difficulties that families cope with, often alone. There is a lack of appreciation of the effect of sleep deprivation on everyone. The reality is that there are so few solutions and answers for families that they can struggle on for many years and are often forgotten about even in close communities, as these challenges become normalised over time - yet the lived experience remains the same.
I do think the hidden aspect of sleep challenges within families is a huge thing. It’s not an obvious thing that people can see from the outside by day, but it can be very dramatic for families by night who want to try and keep life and routines as normal as possible by day to help everyone function at their best!”
- EH, Sibling in the DS Community
The ripple effects of poor sleep are very broad. Tackle sleep issues are a high gain, low risk, and generally low cost intervention, and yet people with Down syndrome do not benefit equally from the sleep interventions that could be offered to them. It’s time to give this invisible issue the attention it deserves, and confront these unequal outcomes.
With gratitude and acknowledgement to the individuals who shared their insights with us. We hope the Down Syndrome and Sleep Research Network will help us move in the right direction towards better outcomes.
Second Annual Conference on Sleep Research and Down Syndrome at the University of Surrey
The Down Syndrome and Sleep Research Network (DSSRN) held a conference of researchers and health professionals on Monday 1st June 2026. Thanks to sponsors, the event was free to attend, and was generously hosted by the University of Surrey. We were delighted to welcome new faces alongside past attendees to our second annual conference.
It was a pleasure to welcome the following keynote speakers:
Dr Shahid Zaman University of Cambridge: The Alzheimer Biomarkers Consortium-Down Syndrome (ABC-DS) study updates
Dr Kiran K G Ravindran | University of SurreySleep Devices in Dementia
Professor Derk-Jan Dijk, Professor of Sleep and Physiology, Director of Surrey Sleep Research Centre: Introduction to the Centre
Dr Ullrich Bartsch University of Surrey: Technology in Sleep Research
Zeke Steer, Milbotix: SmartSocks – Tech Demonstration
Bhaskar Dudem, Z-Pulse: Z-Pulse sleep mat – Tech Demonstration
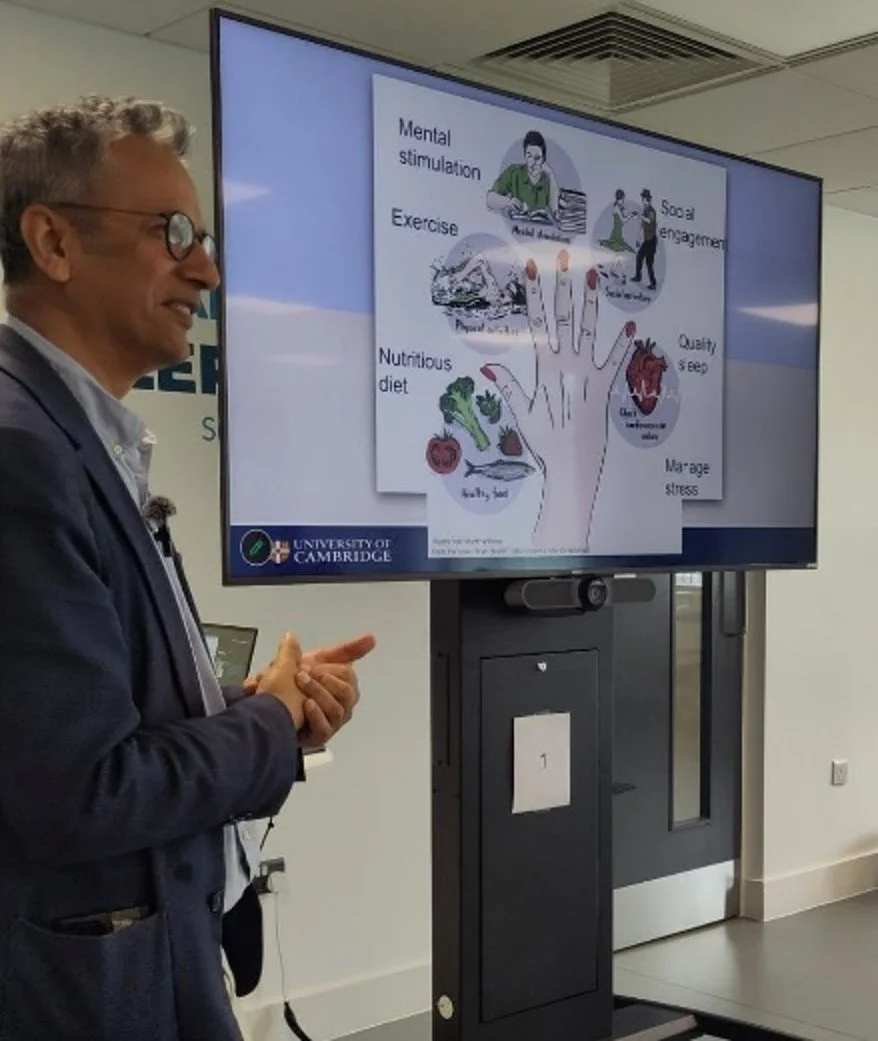
Topics for the conference ranged widely. Sleep is one of various known habits with the power to reduce the risk of developing memory problems, and Dr Shahid Zaman (pictured below) pointed to the fact that such modifiable lifestyle choices are often ignored in favour of medicalised approaches. This has particular implications for the onset of dementia. Dr Zaman described possibilities of improving sleep and therefore outcomes for the DS population, especially with age: “Obstructive Sleep Apnea and fragmentation are modifiable, making sleep a realistic intervention target to delay or soften AD trajectories in DS.”
Director of the Surrey Sleep Research Centre, Professor Derk-Jan Dijk, gave us an overview of his facility’s interest in sleep, and emphasised how complex sleep really is, and how little we understand it. His facility studies aspects such as the intricate connections between sleep quality and daytime behaviour, as well as gene expression, ageing and cognition. Professor Dijk shared: “We’re starting to discover that even small changes in sleep have an impact on daytime function, which I think is actually relevant for many conditions … [sometimes parents say about a child] "He / she is tired. Take a nap." What happens after the nap? Behavior is normalized. Isn't it amazing? But we don't really know what happens during that nap that can change that behaviour so dramatically … there are still a few secrets to be discovered.”
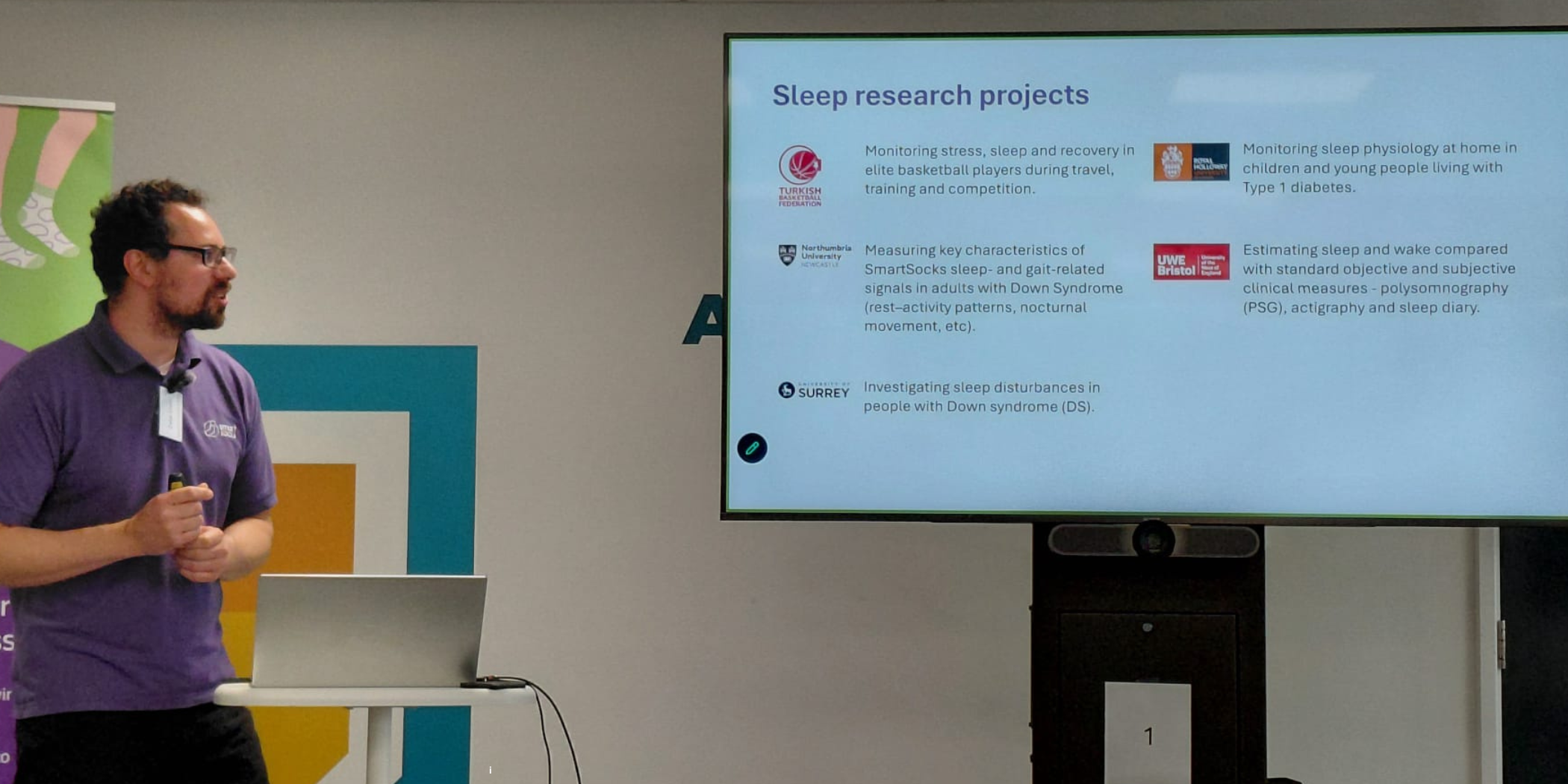
Along with updates from current research projects, we also discussed novel methods of gathering research data and monitoring health, taking a close look at exciting new devices which can help measure sleep and bio feedback, and extend the possibilities for researchers to access meaningful data.
University of Surrey’s Dr Ullrich Bartsch showed various ways that “Sleep technology holds promise to be used as a screening and diagnostic tool in clinical pathways.” There are multiple advantages to appropriate wearables, with different models able to capture different aspects of sleep, and allowing some aspects of sleep studies to take place at home. These technologies can be particularly appealing in the Down syndrome community when they help minimise participant burden.
Conference attendees also had a tour of Surrey Sleep Research Centre’s cutting edge facilities - which one conference participant described as “the most amazing lab I’ve ever seen!”.
In panel discussions, participants initiated explorations of holistic approaches to sleep and attention to other daily lifestyle choices: an area which we are likely to explore further.
Lastly, the DSSRN conference launched a pack of new communication resources by Dr Eve Hirst, a pack designed to help people with Down syndrome understand how to participate in a Sleep Study. This is part of our ongoing aim to improve communication between the Down syndrome community and the research professionals who engage with them. If you would like to receive this pack, please check out this page here: https://dssrn.org.uk/communication-pack
We will keep you informed about further developments for the DSSRN as they unfold!

Speaker Announcement – Dr Shahid Zahman (University of Cambridge) Presenting at June 2026 Second Annual Conference of the Down Syndrome and Sleep Research Network
June 2026 Down Syndrome and Sleep Research Network Conference - register now!
Following last year’s successful inaugural conference where the Down Syndrome and Sleep Research Network was launched, we are delighted to open registration for our second conference. We look forward to bringing together many old and new participants in the area of sleep research in the Down syndrome community. This upcoming DSSRN in-person conference will take place from 10am - 4pm on Monday 1st June 2026, at the Surrey Sleep Research Centre.
Our event will focus on the latest research and advancements in sleep disorders for individuals with Down syndrome. The day will include guest speakers, a tour of the facilities at the Research Centre, and interactive workshops. Building on last year’s presentation by Dr Stephanie Brown from the research team at the University of Cambridge, Dr Shahid Zaman (Assistant Professor) will present on work with The Alzheimer Biomarkers Consortium-Down Syndrome (ABC-DS).
Whether you’re a researcher, healthcare professional, or sleep or DS focused charity, we invite you to join us in advancing the field of DS and sleep research. Together, we can make a lasting impact on the health and well-being of individuals with Down syndrome by addressing one of their most critical needs: sleep. This will be a great opportunity to continue the conversation, share knowledge, and connect with others working in this field.
You can see a playlist of some of our Down Syndrome and Sleep Research resources on Youtube here.
To register for the conference: June 2026 DSSRN Conference registration
We look forward to seeing you again soon!

Sleep Webinar Part 4: What can be done to improve sleep for children with Down’s Syndrome? - Professor Cathy Hill
There are various approaches that can improve sleep practices for children with Down syndrome. Professor Cathy Hill explains some of the most important aspects to consider and opportunities to create improvement.
You can watch this section of the Webinar here on YouTube.
Interventions and Psycho-education
There are some beautiful research projects out there that are looking at ways of managing insomnia in children with neurodevelopmental differences. Most of the work so far has been in children with autism spectrum disorder and children with ADHD, and there have been much smaller projects in children with Down syndrome, but there are some projects out there that have looked at approaches, what we call psycho-education approaches, so working with parents to promote good sleep habits and teach people different tricks of the trade if you like to try and manage some of these really tricky situations at bedtime and they do work.
Evidence for interventions: There have been different ways of doing it – some people do it with a therapist, some people do it with an online website or a digital intervention – and there's been enough work in children with autism that somebody's been able to lump all the research together in something called a meta-analysis, that's just a fancy scientific way of putting all the data together and seeing if there's a truth in amongst the data. Those sort of analyses show that these interventions genuinely do work in children with autism and I certainly from my clinical experience there are a lot of gains that can be made from these approaches as well in children with Down syndrome.
Practical Sleep Hygiene and Habits
I want to skip through some facts about what we call sleep hygiene or what we like to call more commonly now, good sleep habits. So what are the simple things that we can do that help all of us sleep?
The importance of routine: Bedtime routines, it sounds kind of boring, doesn't it? Sounds pretty obvious, but it is the bedrock. It is so, so, so important. Children really benefit from that stepwise sequence of events leading up to bedtime. And the more rigid and the more same it is, the better for the child.
Visual tools and preparation: I've got some pictures there of visual timetables. These things are great for children: countdown timers so that they know they've got 10 minutes before bed or whatever. It's based on classic psychological theory. You learn to associate a sequence of activities with what's going to happen next. I think we have to remember none of us make a sudden transition very easily, do we? We like a little bit of preparation. We like to know what's coming next. We like to prepare ourselves for change. Children are very much the same.
Making bedtime positive: If you can make that positive time as well – and I think most people do intuitively make bedtime a positive time, whether it's a bit of one-to-one time, a bit of quiet time, a bit of story time, whatever the child enjoys. Especially it might be massage; there's all kinds of things that children like, and everybody knows their own child best of all. And building those into the bedtime routine can be very helpful.
The journey to bed: We tend to say, start that journey to bed about an hour before, and using signals and cues that your child understands. Keeping it calm is very important, nothing too exciting. Things that children do in the day help sleep as well, and we know now that exercise is helpful, and the more the better to be honest.
Activity levels and falling asleep: This is a study of school-aged children, a big study of almost 600 children. Every hour a child sat down in the day meant they took three minutes longer to fall asleep at night. So the more active you can get your children, the more likely they are to fall asleep. This is what the UK CMOs (Chief Medical Officers) are recommending now.
Recommendations for active time: It's quite interesting: more than three hours for preschoolers a day, more than an hour a day for five to 11 year olds. Thinking about where we can get that in, it might just be walking home from school rather than taking the car, just building it in; active time outside and in daylight actually as well is really helpful for children wherever you can get it.
Diet and Caffeine
Thinking about children's diet, people don't always realize where caffeine sneaks into food, and caffeine is the best way to keep your child awake, and it can last in your blood and in your system for about six hours. Think about your child's bedtime. We really strongly recommend avoiding things like chocolate or fizzy drinks that have caffeine in;
Caffeine sensitivity and hidden caffeine sources: People know tea and coffee have caffeine in, but look how much you need. For an average five year old, 25 milligrams is enough to stop them going to sleep. A 28 gram bar of dairy milk and they've had 15 milligrams. With a can of Coca-Cola they'll have twice as much as that. So it sneaks in and you don't always realize and there's a big myth around hot chocolate being great for children at bedtime. So we tend to say if your child's struggling to settle to sleep, be rigorous and try and avoid caffeine wherever you can.
The Bedroom Environment
The bedroom environment: keeping it about the right temperature, not too hot, not too cold, 18 degrees is perfect. Keeping it quiet. And the thing with noise is: it's sudden unexpected noises or changes in the background noise that tend to wake us up at night.
Acclimatizing to noise: A continual noise often we just acclimatize to. So children get used to a road noise or a rail track near the house, things that they're familiar with, the drone of airplanes overhead. We don't tend to wake up once we're used to those things, but sudden intermittent noises like a telephone ringing or or a voice, this sort of thing will wake children up.
Lighting and melatonin: Dark is so important. So the journey to bedtime, get those lights dimmed. If you've got a child that's afraid of the dark, that's very common, try to use a night light and try to have an orange or red night light, not a white one. Because white light or blue light stop our body making the sleepy hormone melatonin. And screens, of course – all those lovely tablets that we've got now, phones, TV screens – they spit out blue light and they stop our bodies making melatonin.
Melatonin and rest: Melatonin helps ease us into sleep and it's incredibly important.
So dim light and red light or plug in orange lights if your child wants a bit of light to reassure them at night.
Lying down: I think we all kind of intuitively know that a bed is helpful and being comfortable and being horizontal is helpful, although in some cultures people sleep semi-seated. There's all kinds of different ways of doing it, but most of us like to sleep horizontally. Not too stimulating.
Boring is better:I think often we make the mistake as parents to think, "My child's not sleeping, I've got to make the bedroom nicer." If the bedroom's nice, if I paint the walls this way or if there's nice toys in there, it's a lovely place, then my child will sleep.
And of course, it's a kind of confusing message sometimes for a child. So actually a boring bedroom is the best kind of bedroom to sleep in.
Sleep safety: And safety, of course, is extremely important. If you've got a child that might climb out the window, you want window locks. If you've got a child that might run around with a night terror or a sleepwalking, you want to make sure the house is nice and safe.
Shared spaces: And we tend to say, if your child struggles to understand bedtime, if your child has learning disabilities that makes that difficult to understand, I think having a bedroom that's also a play centre in the day is confusing, that you're going to this space again but now you've got to do something different.
So we tend to say to parents, if your home doesn't have the capacity to separate out that space, put the toys in a little box and wheel it out. All those tempting things aren't there anymore; just comfort toys that children might need to sleep is all that's needed.
Visual examples: And to make you think, there's a wonderful book about where children sleep around the world, and just look at some of these images. That's an example of a bedroom that's not great for sleep. Stuffed full of toys and entertainment. So, would you go to sleep in there? I think it would be kind of challenging, wouldn't it?

Electronics in the bedroom: And this one, if you have a quick squint around, look at all the electronics. A lot of electronics in the bedroom. We know that electronics have huge benefits for children in terms of learning and lots of children are soothed by electronics, but as I say, we do have this real problem of blue light and accessibility.
If it's there at 3:00 in the morning when you wake up, it's too tempting to want to hop on and have a look.

Parental challenges: It's very tempting as parents to think, "Well okay, it soothes the child, whatever gets a night's sleep, let's leave it be." So, I think we have a real challenge in this day and age around accessible tablets and electronics.
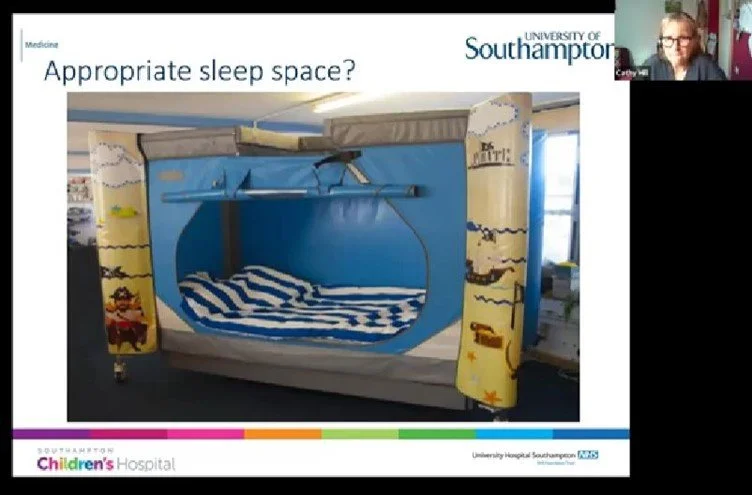
The simple sleep space:And I'm putting that up there because there's an increasing vogue for sleep pods. And actually, as intelligent adults, people pay money to pop into these. This is actually all you need, isn't it? In real life, that's all you need to sleep. A door. Safe comfortable space. So have a little bit of a think about what we're doing sometimes to our children's bedrooms.
Safety sleepers: And for many children, safety sleepers and there's a whole bunch and variety of them out there can be a helpful way of keeping a child safe at bedtime and actually giving a beautiful clear message. This is your lovely safe sleep space. This is where you go to sleep. It's not a play space. So for some children that kind of a sleep space can be very helpful.
Screens and Physical Health Issues
I've talked about screens: I won't labour this, but there's loads of data now showing that more time on screens, even in toddlers and preschoolers, it knocks their nighttime sleep and they take longer to fall asleep. And in school age children, they're more likely to be sleepy in the day and to not have enough sleep at night.
Finding balance: It's not a myth, it's not kind of PC, goodie-two-shoes-people who think ‘keep your children off screens’: it really does make a difference. So we have got to find that delicate balance between all the wonderful, wonderful benefits of screens and keeping the time reasonable. It might be because sometimes children are using the screens instead of going to sleep. It might be that they're too stimulating at bedtime, but we know that light has a big effect.
Underlying medical issues: I think we do have to pay a little bit of attention to things like pain, medical problems like gastroesophageal reflux – if a child's refluxing up their tummy contents and they've got a sore gullet, that's going to make it hard when you lie down flat. Is your child hungry? Has your child had their sensory needs met?
These are all important questions to ask. So here we go.
The sleep jigsaw: It's a bit of a jigsaw puzzle, isn't it, sleep? So to do it well, we've got to be in the right environment, or it helps at the very least. But that's the bedroom environment, but also the child's internal environment. Are they calm? Are they comfortable? Are they free of pain? Are they satiated but not too full of food? You need to be tired, that's self-evident, and your body clock needs to be on the right time zone.
And once all those things are all beautifully lined up, you've actually got to make a positive choice to go to bed because you can make a positive choice not to. We can all decide not to go to bed on any one particular night, even if we're absolutely dead dog tired.
DSSRN March 2026 Webinar Available Online
The DSSRN held its first ever online meeting on Monday 23rd March 2026, bringing together researchers and practitioners focused on sleep and Down syndrome. The meeting centred on creating the right conditions for better coproduction and inclusion in sleep research for people who have Down syndrome. A recording of the presentation is available here.
Participants joined the meeting from various international locations including England, Scotland, Ireland, the United States, Brazil and Belgium. A wide range of research organisations, practitioners of various disciplines, and charities were represented at the lunchtime webinar. The DSSRN was created as a bridge between individuals and groups who have excellent practices and expertise to offer, and newcomers to the practice of including people with Down syndrome and other learning disabilities in sleep research. Both ends of the spectrum of expertise were well represented: some with pressing questions, and others with excellent answers. It was encouraging to see resources and recommendations being shared between participants at the meeting.
The Network aims to accelerate sleep research by bringing the right experts together, acting as a catalyst for creating better resources and practices. We also want to help develop and mentor a gold standard for coproduction and inclusion of people with Down syndrome, which can be implemented by researchers and practitioners. One of our aims is to foster centres of excellence where people with Down syndrome have a real voice in the process of research.
Creating and reviewing resources to explain sleep studies
An excellent presentation was made by our good friend Dr Eve Hirst and her brother Joshua, who had co-produced materials for the meeting.Joshua created, wrote, directed and presented a video about a recent trip to hospital from his lived experience as a person with Down Syndrome, and the presenting team discussed how Joshua prepares for medical procedures, including watching and also creating videos about the experience.
Since sleep disturbances are so common in the Down syndrome community, the likelihood that someone with Down syndrome will need to do a sleep study in their lifetime is much higher compared to typically developing individuals. Despite this, few resources exist to make sure that everyone is communicating clearly, and there is a scarcity of aids to understanding comfortably what is going to happen. It’s a big gap that makes it hard for both sides: researchers and research participants.
Followers of the DSSRN will be aware that Dr Eve Hirst has been developing a suite of tools to help researchers involve and communicate more effectively with people who have Down syndrome, and some of these new resources were showcased at the webinar. Soon, we hope that when people with Down syndrome need to have a sleep study, they can read, watch or listen to such custom-made materials that explain what to expect, and what the sleep study will look like. It was widely agreed at the webinar that these materials would be helpful to use in many settings.
Focus Group Needed
We are forming a focus group to review the communication pack before it is launched. We need a panel of experts by experience who have Down syndrome, and also carers, to help us review the materials. We are looking for 10 participants to take part in this focus group, to review and discuss the material. Do you know anyone who would like to be involved? You can also bring someone to support you to this meeting.
The upcoming focus group will take place on Wednesday 29th April at 7pm UK time. International participation is welcomed. Please email info@dssrn.org.uk to register.
Please see the easy-read invitation below. We would be grateful if you could bring it to the attention of someone in the Down syndrome community who would be interested to help us.
Stay tuned for upcoming announcements about:
- The planned launch of the resource pack
- The next in-person meeting of the Down Syndrome and Sleep Research Network, and how professionals and researchers can register

Sleep Webinar Part 3: Sleep and Down’s Syndrome: What’s going on? Why should we address sleep problems? - Professor Cathy Hill
There are many implications that flow from sleep deprivation for individuals with Down syndrome, particularly for young children. In this segment, Professor Cathy Hill explores common issues, consequences, and the compelling reasons to identify and address sleep problems.
You can watch this section of the Webinar here on YouTube.
Classifying Sleep Disorders
What's going on? Parents are telling us there are problems: children are not sleeping as long and waking up more. What is this all about?
The importance of diagnosis: We have to find a cause. You can only really manage and treat something if you know what the cause is. In sleep medicine, we work to this classification. People often think, "My child has a sleep problem, I need to fix it," but they don't think about what is causing it.
There's a whole bunch of different reasons. When I teach doctors about sleep, I say: if you have a cough, you don't treat the cough: you try and find out if it's asthma, a chest infection, or a tickly throat. They are all very different and will have different treatments. Exactly the same is true for sleep disorders.
Common sleep disorders:
Here are the kinds of things we're looking at:
- breathing problems at night;
- insomnia (difficulty falling asleep and staying asleep);
- being too sleepy in the day (rare disorders like narcolepsy);
- parasomnias (like sleep terrors and sleepwalking);
- circadian rhythm disorders (where the body clock is not working properly);
- and movement disorders of sleep.
My trick is trying to unpick what's going on, because many of these things present in exactly the same way: cannot go to sleep, cannot stay asleep, and too tired in the day.
All of these things may potentially be involved.
Understanding Insomnia: Sleep Onset Association Disorder
I'm going to talk first about insomnia. It is the most common sleep disorder we see in children. No matter what the underlying developmental issues or medical problems might be, insomnia is very often part of what we are seeing.
Habits and environment: One that might be familiar to you is the most common insomnia we see, and it has a fancy long name: sleep onset association disorder.
The concept is that every single one of us on this planet learns to fall asleep or has a preference for falling asleep in a very particular environment. Stop and think for a second: when you settle yourself down to sleep, in those ten to fifteen minutes before you go to bed, I bet you do something rather similar every night. Most of you will have a habit. You like your bedroom a certain way, the lighting a certain way, or maybe you want the radio on. You'll probably put yourself into a particular position in bed.
The pillow analogy: Once that is all good, it makes it a wee bit easier to fall asleep; you've learned that association. Most of us in the Western world have pillows, don't we?
That is a cultural thing we do – not all over the world, but we tend to have a pillow.
You're in your bed, you've got your pillow, and you settle down to sleep. Imagine you wake up after your natural night waking – you had fallen asleep, everything's good, you had your pillow. Then you have your first natural night waking; we all do it, probably every hour after that first nice chunk of deep sleep. But your pillow is gone. You're not going to go back to sleep. You're going to feel quite anxious, things will feel strange, and your bed will feel odd.
The anxiety of change: This is the idea behind sleep onset association disorder. Many parents and children develop a habit around settling the child to sleep. I have done it as a parent, and many parents I see do it. We put a lot of effort into getting our child to sleep, which might mean rocking, cuddling, soothing, musical toys, lights, or warm milk. They often work fantastically well, and the child goes to sleep beautifully.
The waking dilemma: The problem is when you have that first night waking: the rocking isn't there anymore, the music isn't there anymore, and the lights are gone. You're not going to be able to fall asleep again because your metaphorical pillow has gone. So what does the child do? They're not comfortable and cannot go back to sleep because this isn't how they fall asleep. They're going to shout for mom or dad or come out of the room. The parents are going to go in and do the whole thing all over again. That might sound familiar to some of you, but it is the most common sleep disorder we see.
Learning to self-soothe: One simple tool of the trade – and I think every parent and antenatal class should be taught about this – is that at the right time in a child's development, you encourage and help the child to learn to self-soothe themselves to sleep. It is never too late, even in the teenage years. Settling to sleep should be a lovely, soothing process; it does not have to be harsh or scary. In fact, it absolutely shouldn't be.
Independent sleep (and co-sleeping): The point is that the child settles in their bed independently, sleepy but not quite asleep yet, and the parent hopefully exits the room. Assuming you don't want to co-sleep; if you want to co-sleep, that is absolutely fine and that is your choice. It is quite culturally common in the UK for people to want their children to sleep independently. I'm a big believer in flexibility – every family and culture is different – but I think understanding this little association is very helpful and can be a big clue for people to move forward.
Limit-Setting and Consistency
The other type is the limit-setting type, and they often mix together. In this one, instead of lots of waking, children struggle to fall asleep. Parents will say, "It's a nightmare getting this child to bed." There is screaming and shouting; they might be sick or very upset, and they are up and down the stairs, very unhappy about going to bed. The same happens at night waking, so the problems are at both ends.
The gambling phenomenon: We are all human, and children respond to consistency, but in real life it is hard to be consistent, especially if you are exhausted. We call this the gambling phenomenon – like old-fashioned fruit machines. If the third time you pull the handle, the money pours out, you're going to think it's fantastic and keep playing.
If a child is very unhappy about going to bed – and this is not an anxious or ill child, but a feisty, strong child who knows they can put up a good fight to get what they want – they're going to keep pushing that fight. They know if they keep pulling the handle – in other words, keep asking – they'll get what they want. That is so difficult for parents who are very tired, but consistency in approaching this is terribly important.
Research Findings on Sleep in Young Children
We did some research a few years ago with over 202 families across the country in Southampton and Sheffield. Some of you may have been involved. We were looking at sleep and breathing in infants and toddlers under two years.
Comparative study data: 140 families completed a questionnaire about sleep behaviours. We were able to compare them to a study conducted by a psychologist in the US who gathered data in the UK. We wanted UK children to compare to our group of children with Down syndrome. She had a group of 489 children where families answered the exact same questionnaire. We could match by gender and age and look at the differences. Parents told us about how their child slept and how they settled them to sleep at the beginning of the night and during night wakings.
Striking differences: We found some striking differences in children with Down syndrome. First, parents were much more likely to say they had sleep problems: 45% compared to 19% of the non-Down syndrome children. They were much more likely to snore, which was no big surprise because we know that is an issue.
Sleep loss statistics: The very shocking thing for me was that they had 55 minutes less sleep at night than their typically developing peers. Remember I was saying that at 45 minutes you see very big differences in children; 55 minutes is a big difference. They were shifting some of their nighttime sleep into the day with more naps, but even adding those in, they were still having almost 40 minutes less sleep in 24 hours. This was a real difference in total sleep time. They were approximately twice as likely to have problems settling to sleep.
Settling behaviours: So then there's the big "why" question. The study was observational, so we couldn't truly answer that in detail, but we could get some clues from the questionnaires. Parents of children with Down syndrome were more likely to bottle-feed their child to sleep (almost five times as likely) or to be rocking or holding them (almost six times as likely). They were also more likely to have a parent lying alongside them or to be in the parent's bed to settle. We put all that together and found parents were a bit more than four times more likely to be with their child at the point they settled.
Engagement in settling: In the non-Down syndrome group, about 25% of parents were still involved in settling because these are young children. However, it was much more striking in the children with Down syndrome. The received wisdom in medical literature is a bit of a simple interpretation: people think the biggest problem is sleep apnea, so surely all sleep problems are to do with that.
Snoring vs. settling behaviour: This study said something slightly different regarding why we were seeing shorter sleep. Remember that number of 40 minutes less sleep across 24 hours. We looked to see whether snoring explained the difference. Snoring didn't affect any aspects of sleep other than night waking, which you would expect.
Whether or not the mom or dad were there when the child settled to sleep explained later bedtimes, more frequent and longer night wakings, and shorter periods of uninterrupted sleep.
Impact on total sleep: We know now that the more consolidated sleep you have, the better your sleep is. Once we looked at this, it actually explained an hour less of sleep overall. If the parents were very engaged in the child's settling, those children had around an hour less sleep overall.
Causal direction: Is that chicken or egg? I talked about the sleep-onset association, and it sounds a bit like I'm pointing the finger of blame, doesn't it? But it could be the other way around: if you have a child who is inherently difficult to settle for some other reason, you're going to respond in a different way.
Individual temperaments: Quite often I see children where there are multiple siblings, and this particular child is different. All children have different personalities, temperaments, and needs, and that can drive the dance between the parent and child and how those behaviours play out in the night. So, we don't know that from this research. It wasn't designed to tell us that one way or another. But if we look at the other literature in typically developing children, we absolutely know that parent behaviour at bedtime will affect how a child settles and how a child manages their natural night wakings.
The magic skill of self-soothing: And we know as I've mentioned that all of those lovely strategies like rocking and very what I think of as effortful settling, working hard to get your child to sleep: they're very effective, they get the child to sleep, but the child hasn't learned that magic skill to self-soothe at night and struggles then when they wake up. And as I've said, all of these things sound very simple, but actually in real life it's more complex, isn't it?
Cultural and emotional factors: Because we all have our cultural norms, how you were settled as a child, the kind of routine that you had, your beliefs about your child. I think a powerful important belief is if you see your child as unwell or fragile, or if they are unwell, if you've had a child who's had a difficult first year of life, if they've had cardiac surgery, if you've had a difficult stressful time - it's damn difficult to switch the light off and say, "Night, night, I'm sorry, time for bed." Now that is very difficult to do: it's much more human and natural to want to cradle and rock your child. So these things are quite complex. And as I said, it'll depend on a child's temperament as well and they're all different, aren't they?
Independent impacts on sleep: And of course we know as well that children with Down syndrome are at more risk of things like autism spectrum disorder and problems like ADHD, and those things all have independent impacts on sleep and bedtime.
Next in segment four: what other interventions can improve sleep quality and quantity for children with Down syndrome? Professor Cathy Hill describes additional practical habits and approaches.
Calling all DS Sleep Researchers and Professionals: Dr Eve Hirst as Keynote Speaker for next meeting of the Down Syndrome and Sleep Research Network
The next meeting of the Down Syndrome and Sleep Research Network (DSSRN) is now set to take place online on Monday 23rd March 2026, from 12 noon to 1:30 pm (GMT).
The theme will centre on making research and clinical information accessible to people with Down syndrome. We are delighted to welcome our keynote speaker, Dr Eve Hirst, winner of the 2021 Research, Innovation and Education Award, who is developing new materials for the DSSRN. Dr Hirst will present in collaboration with a co-producer with lived experience of Down syndrome, offering first-hand insight into practical sleep and hospital experience, and providing examples of helpful and unhelpful practice.
We’ve chosen this topic because ensuring high quality two-way communication with people who have intellectual disabilities is at the heart of this kind of research. We know that this approach better protects human rights and equity, ensures effective co-production, reduces frustration, and makes for much better science. We’re all agreed that it’s incredibly important – but on a practical level, how can we practice it and promote it?
We hope this meeting will provide tools, insights and resources, as well as peer support. The session will be interactive, focusing on practical implementation and how to incorporate these resources into practice. The meeting will focus on co-production, accessible materials, and service user involvement.
We will also provide updates on the next in-person meeting of the DSSRN which will take place in summer 2026.
The registration link for the digital meeting is here. The link will go live at 12 noon GMT on Monday 23rd March 2026. You can also register via the QR code below.
Please spread the word to others who would be interested and would benefit from this meeting, especially if they are not already connected to the DSSRN.
We look forward to seeing you online then!

The DSSRN is grateful for the support of the Trisomy 21 Research Society in making this event possible.


Sleep Webinar Part 2: Understanding Sleep is Key: Professor Cathy Hill
An introduction to sleep: what it involves, and what is needed for healthy sleep patterns.
Note: This series of blogs are drawn from an online seminar that was held on June 30th 2021. It featured the excellent research of Professor Cathy Hill, Dr Rina Cianfaglione, and Dr Lizzie Hill. The live seminar was very well attended, demonstrating a very high level of interest on the topic of sleep and Down’s syndrome. It is presented here in blog format, edited for clarity. To watch the original presentation with visual slides, you can watch here in full, or via the video segments that are linked with each blog.
You can watch this section of the Webinar here on YouTube.
Introduction and Welcome
Dr Corcoran: I would like to invite Dr. Cathy Hill up on the stage. Welcome, Kathy. It is so good to have you here today.
Professor Cathy Hill: I like the idea of the stage. I have been talking to myself in my office! It is actually lovely to see some faces. Thank you to those of you who are brave enough to put your cameras on. It makes it so much more real than sitting and talking to a screen. It is fantastic that so many people have joined. I know when Lizzie proposed this, I had no idea we were going to have so many people interested, and that is great. I think that speaks volumes about how important sleep is to children and to families. Certainly, that is my lived experience.
Dr Liz Corcoran: To introduce you, Dr. Hill is down in Southampton. You are an associate professor of child health within the university medical school there. Obviously, your focus is on sleep, and you definitely have a heart for our community. You have done a few research projects on children with Down syndrome to work on understanding sleep better, and you would love to do more, and we would love to see that happen. So, I will get out of your way and let you begin telling us a little bit about sleep in Down syndrome.
Professor Cathy Hill: Thank you to the kind parents who shared this beautiful photograph of these two gorgeous twin boys. What a lovely image. I have stolen it and put it on the header slide because I thought it was such a great image. Thank you, Liz, for that lovely introduction.
Presentation scope: As Liz said, I have been really interested in sleep generally in children with Down syndrome now for about ten years. What I want to do today is to talk about sleep in general. When Liz said, "Let's talk about sleep," I thought, "Gosh, which bit of the ten hours of talks am I going to give on this?" because there is so much we could talk about. It is such an interesting area. So, I hope I hit the spot today and focus on things that are relevant to you.
Clinical experience: My interest is very much inspired by my clinical work. As well as doing research, I am a pediatrician and I run a sleep clinic where we have around 500 referrals a year; amongst the children we see are quite a few children with Down syndrome with a variety of different sleep problems.
The Basics of Sleep Physiology
Understanding physiology: First of all, I think sleep is quite poorly understood.
I think we cannot really understand why children have sleep problems and what those problems are about unless we have some fundamental understanding about sleep physiology – basics as to what sleep is and what is happening.
The importance of sleep: It may not surprise you, but even in medical school, we teach very little about sleep. I am sure this was Liz's experience and it was certainly my experience. Yet when you think about that in the context of children: children spend half of their breathing hours asleep. There has to be something jolly important happening in the body and in the brain during that time for us to spend all that time in this level of altered consciousness.
States of the brain: I am going to show you a few images to cue you in a little bit about some key facts about sleep. I think most of you will probably appreciate that sleep is not one thing. It is fundamentally a state of the brain. It dictates your whole body physiology.
Depending on what state of sleep you are in, different things are happening throughout your body with your hormones, your heart, your breathing, and your temperature control. It affects just about every aspect of your bodily functions. As I said, sleep is not one thing; it is a whole series of different brain states. This is a little diagram illustrating what that looks like.
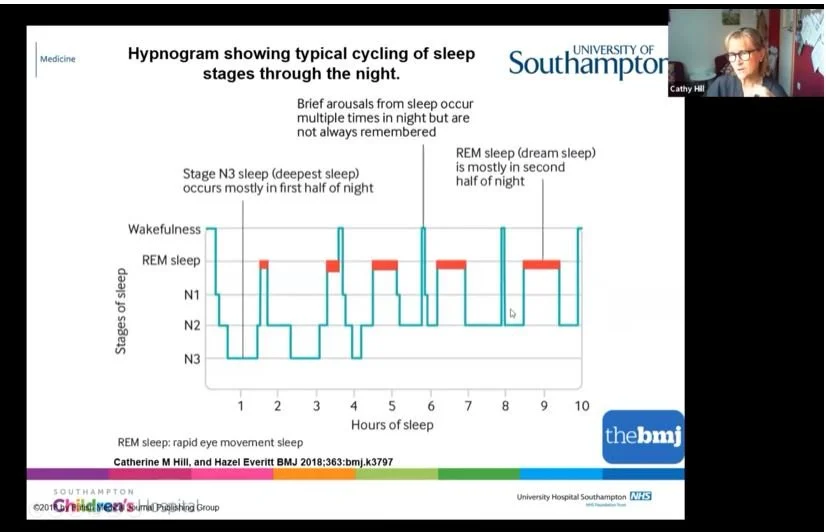
The sleep journey: During the night, your brain takes a journey through the landscape of sleep. We start off in wakefulness at the top and progress quite rapidly. For children or adults who fall asleep easily, off we go into the journey of sleep.
Deep sleep: The first bit of sleep we hit quite quickly is our deep sleep, and it is called deep sleep because it is actually hardest to wake up from. Many parents say to me, "It might be a real struggle to get my child to sleep, but once they are asleep, we know we have that precious little hour when they are going to be quiet." That is because they are sitting there in their deep sleep. You can see that deep sleep is mostly in the first few hours of the night.
Dream sleep: Very often parents will say they are quite settled at the beginning of the night, but then it all changes as the night goes on. The reason it changes is that as you progress through the night – you can see these red lines here – this is dream sleep.
You have more and more dream sleep as the night goes on.
Fragility of sleep: Dream sleep, contrary to what people often think, is actually very fragile. It is a sleep you can easily wake up from, and that is why we remember our dreams sometimes if we wake up out of them. As you go through the night, your sleep gets lighter; so, stage three sleep is deeper, and as we go, it becomes lighter sleep.
Normal night wakings: Basically, as the child goes through a night's sleep, they are more and more likely to wake up. In fact, we have natural wake-ups about once an hour after our deep sleep is done at the beginning of the night. A very important message is that waking up at night is normal. We all do it multiple times. It is usually quite brief and we do not always remember it. A lot of us might remember waking up and checking the clock – great, it is 3 o'clock – and we might get up and go to the loo. Children do this as well. A lot of the problems that children have with night waking relate to these natural night wakings that then follow on to a behaviour, and we are going to come back to that in a minute.
Muscle control in sleep: Another little fact I want you to grasp at this point is that everything in your body is different during the different sleep stages. That includes our muscle control. An important thing to be aware of is that in dream sleep, we switch our muscles off; we effectively become paralyzed from the neck down. That stops us running around the room and acting our dreams out.
Floppy sleep: This becomes important when we talk later about sleep apnea because it means that all of our muscles, including the muscles at the back of our throat, become a little bit floppy. So, hold onto that little fact as we go through: dream sleep equals floppy sleep because we are paralyzed.
How Much Sleep is Needed?
I think the question I am probably asked most often by parents is, "How much sleep should my child have?" The answer is: as much sleep as they need. It is a very difficult one to answer because every child is different.
Sleep guidelines: This is an interesting graphic that shows ideal amounts of sleep (dark blue blobs), what might be okay (turquoise blobs), and the bit that probably is not okay (red blobs). As you can see, it changes through life. When children are born, they need a lot of sleep – we all know that. As you progress through life into the teenage years, you need less and less sleep.
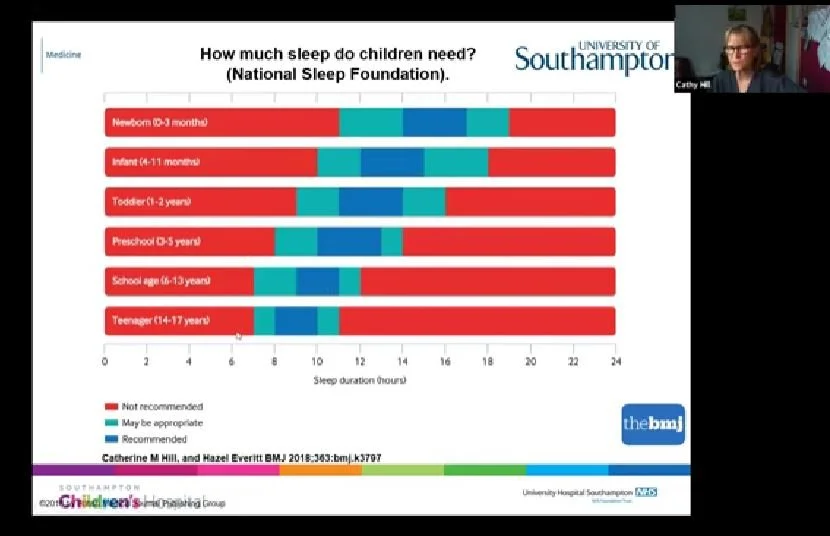
Variation by age: Pretty typical for a teenager might be about nine hours, and for a school-aged child it might be around ten hours, but as you can see, there is huge variation around this.
These figures were not derived from somebody guessing and plucking numbers out of the air. This was from reviewing 700 research papers and looking at the associations between how much sleep children had and what happened to them – their physical health, their mental health, and their ability to think and stay on task. So it came from science; it is not absolute, but it is a kind of guide.
Measuring enough sleep: There is a huge amount of variation. The bottom line is, if your child can ping out of bed in the morning feeling reasonably refreshed and does not show signs of tiredness in the day, chances are they are getting enough sleep. It is quite a tricky one to measure. Of course, what we know with children is that, unlike adults, they do not just look sleepy. Quite often they become dysregulated, their behaviour goes off, and they are more hyperactive or more challenging; that can be a sign of sleepiness in children. It can be very confusing and difficult to spot sleepiness in children.
Factors That Influence Falling Asleep
What makes us go to sleep? We all imagine it is this magic process where there is like a switch in your brain and you just go to sleep. It feels like it should be natural – something we can just do without really thinking about it. Surprisingly, it then becomes very frustrating if we cannot or if our children cannot.
Brain readiness and age-appropriate bedtimes: I want you to think about some of the key things that have to be right and lined up in order to go to sleep. First of all, your brain has to be ready for sleep. What does that mean? That means you have to be tired. You might think, "This isn't much of a lecture, that's pretty obvious, isn't it?" However, it is not always obvious to people. I have come across many parents, particularly when children have learning disabilities or physical challenges, who might put their child to bed a wee bit too early and haven't thought, "Well, actually, my child is now 15." Your typical 15-year-old goes to bed much later; they are not going to be going to sleep at 7:00 in the evening anymore like a younger child might.
We have to be tired, which means we have to have been awake for long enough to have that brain urge and brain readiness for sleep.
The body clock: The other thing that's perhaps a little less obvious is our body clock – our endogenous body clock – which sits deep in our brain and tells us approximately when we want to go to sleep. That peaks at about 3:00 in the morning; so, if you are trying to do an all-nighter or a night shift, that is the time when it is hardest to stay awake. If your body clock is completely out, which it can be in some sleep disorders, it is very hard to go to sleep even if you are tired. That is what happens when we get jet lag.
Relaxation and calm: As well as your brain being ready, we also have to be relaxed and calm. We all know this from lived experience. If you have any worries, if you go to bed stewing about something, or if you are stressed because you have to get up early to catch a train, it is much harder to fall asleep. For children, that can be very relevant if they are hyped up, anxious, phobic about school, or fearful; it is much harder for them to settle to sleep.
Physical and sensory needs: The physical environment needs to be right, and we are going to talk a bit about what that involves. Of course, you have to be free from pain. We see a lot of children who have particular sensory needs. Have those sensory needs been met in the run-up to bedtime over the day, and are their sensory needs being met in bed?
Temperature and hunger: You have to be the right temperature – not too hot and not too cold – and it helps if you are not hungry. It equally helps if you are not full of food because a big meal or a big tube feed just before you go to bed is going to make it much harder. Your body naturally slows down its gut digestion during sleep, so it helps not to have a full tummy when you go to bed.
The choice to go to bed: This is the one that people forget about: we all make a choice to go to bed, don't we? After about four days of trying to stay awake, you lose that choice and it becomes involuntary. But we all make a conscious choice that it is now time for me to go to bed.
So, there is a huge cognitive and behavioural aspect about going to sleep. That is very much true for children as well. That is where some of the things you can do can be very helpful to help the child be in the right cognitive state of readiness for going to bed.
Common Sleep Challenges in Down Syndrome
Through the research over the years, what have parents told researchers about children with Down syndrome and their sleep? There is a famous, well-known sleep questionnaire that is often used, and I have pulled all the data across hundreds of children.
Bedtime resistance: These children are more likely to be resistant at bedtime than their non-Down syndrome peers. Resistance is very much about behaviour – not being happy to go to bed, not wanting to go to bed, or putting up a fight about it. They are more likely to be anxious about going to bed.
Waking and restlessness: They are more likely to wake at night and more likely to have problems with breathing at night. They are more likely to be restless. I hear this so much. "My child is very restless, tossing and turning, throwing the sheets off, upside down, left, back to front, all over the bed, moving around." Some of that is about rocking at night.
Daytime sleepiness: They are more likely to be sleepy in the day, which is a real red flag because, as I mentioned, children tend to go a little hyper before they actually become sleepy. Sleepy children really do tend to be properly sleep-deprived children.
Objective measurements: There have been studies that use what I call objective measures. They use equipment and monitoring to look at what's different about sleep in children with Down syndrome. Here is what those research studies have shown. First of all, thinking about actigraphy: this is the fancy medical word for a kind of Fitbit you or the child wears at night that measures movement and downloads it into software so we can guess when the child is sleeping and when they are awake.
Poorer quality sleep: What we see is shorter sleep and poorer quality sleep, with a lot more interruptions and night wakings. When we put children into sleep laboratories, where we look at brain waves, sleep states, and sleep stages, the data isn't very consistent, to be honest. Some studies say one thing and some say the opposite.
But there is a common thread running through this: if there is one feature that is seen more consistently, it is less dream sleep. I'll come back to that later. Some of you might be asking why that is.
Importance of Sleep for Development and Health
Are we bothered? Every parent who cannot get a good night's sleep is bothered and does not need to be told this is important, because you know yourself what it feels like not to sleep.
Research in development: However, there is some fabulous research now that tells us why sleep is important for child development and health. I could spend hours talking about it, but I'll give you some headlines.
Experimental sleep restriction: This is about typically developing children. There have been some very smart studies called experimental studies. This is when you take a group of children and expose them to sleep restriction. They have a few nights when they do not have enough sleep and some nights when they have normal sleep, and you spot the difference. You are comparing the same child between good sleep and bad sleep.
Impact on attention: Those studies show that children very rapidly – even over three days, and I am not talking about crazy all-nighters, but maybe 45 minutes less sleep a night – show a difference in how well they can stay on task and pay attention, how well they can control their behaviour and emotions, and how restless and impulsive they are in the day. That's from a really small amount of sleep deprivation. Think about that over a long period of time and what it does to children and their ability to learn in class if they are restless and cannot pay attention.
Physical health risks: If you follow children up over time, we know a whole load of stuff can happen. We know you are much more likely to be overweight and obese if you have short sleep, even in early childhood. We did some studies here in Southampton looking at children when they were three and measuring body fat mass; children who weren't sleeping enough at three were much more likely to have a lot more fat in their body at age six.
Brain development: Stunning data in long-term studies has shown that not having enough sleep in the early years can even affect how your grey matter, your clever brain, develops. That's very new and exciting data because if there were one reason why children should sleep, it's for their brain development.
We have to ask ourselves why little babies sleep so much. What's going on that means babies need to sleep so much while we need to sleep less and less as we get older? It probably is related to brain development.
Research in Down syndrome: But what about children with Down syndrome? As Liz said, the research often follows later because it is harder to get funding for this kind of work. From my own experience, we have had absolutely fantastic support from parents; that has never been an issue. Once you get the funding and a project up and going, we've had some really fabulous support from parents in the past, volunteering their children to take part in research, which is great.
Language and behaviour: What do we know? We know there's an association in little children – this was some fabulous work from Arizona – between short sleep and both daytime behaviours and language development. Compared to the thousands of children studied without Down syndrome, the numbers are still low regarding how it impacts daytime well-being and behaviour.
Cognitive reserve: But I've always argued that children with Down syndrome have less "cognitive reserve" to call on. If you already start with some learning challenges and then throw another challenge in like not getting enough sleep, you haven't got as much reserve there. If we were able to do the same amount of research as has been done for typically developing children, I think those effects might even be greater.
Upcoming: Part three focuses on how children with Down syndrome experience sleep, and what research specific to Down syndrome tells us about this.

Developing communication resources about sleep studies for individuals with learning disabilities
With thanks to Dr Eve Hirst for her message on the importance of adapted communication for people with Down syndrome.
One potential barrier to working more effectively with the Down syndrome community is the scarce availability of tools for high quality two-way communication.
People with Down syndrome have differing degrees of learning disabilities, ranging from mild to severe, which can make it more difficult for individuals to communicate their needs, and also present challenges for practitioners who may not be fully trained in appropriate communication styles.
The DSSRN is very happy to be working with Dr Eve Hirst on developing and distributing new resources, including sign supported videos and social stories, designed to simplify complex health conditions, investigations and procedures.
We are developing an accessible resource pack to communicate the importance of sleep studies. This will consist of an easy-read written resource, Makaton symbol-supported information, and Makaton sign-supported video.
Dr Hirst is passionate about improving communication in medical contexts for people who have intellectual disabilities. She is a Makaton tutor and also a Signalong Tutor, has two siblings who have Down syndrome, and she teaches other medical professionals to use Augmentative and Alternative Communication (AAC) to better support their patients.
Dr Hirst says: “We know that communication is essential to delivering good quality, safe, and dignified care to our patients. If we can adapt our communication to meet the needs of the individual in front of us, I firmly believe we can make a practical and palpable difference to the health inequalities experienced by people with a learning disability, such as those with Down syndrome.
I encourage all health professionals, if you haven’t already, to look locally to your hospital, trust, or region for training in multi-modal communication, such as Makaton. This will equip you with the expertise, such as learning to use signs, or gestures, and symbols, to communicate effectively with patients you encounter who rely on these tools to understand and be understood, and give these patients the time and the space to advocate for themselves.”
Dr Hirst was the winner of the Research, Innovation and Education Award at the Northern Care Alliance Staff Awards 2021. She designed and co-led the roll-out of an interactive Signalong training program for her colleagues in Oldham hospital’s adult and paediatric A&E departments. The Oldham project won two awards: the 'Oldham Care Organisation Award for Research, Innovation and Education', as well as the Northern Care Alliance award for the same. The project was also shortlisted for the Greater Manchester Health and Care Champion awards for the 'Equality' category.
If you are a health professional wanting to learn Makaton/Signalong in your workplace, please feel free to contact Eve: eve.hirst@doctors.org.uk
You can find out more about Makaton here: www.makaton.org
Further updates to come!

Down Syndrome Awareness Month October 2025: Dr Goffredina Spano on sleep as a missing piece in Down syndrome research
Thanks to Dr Spano for this message during Down Syndrome Awareness Month.
I'm Goffredina Spano, I'm a senior lecturer at Kingstown University. My research program explores the relationship between sleep and different outcomes, including cognition in different neurodevelopmental conditions, including Down syndrome.
My journey with Down syndrome started long time ago in 2004, when Julia was born. During that time, I was doing my Masters in psychology, and I was trying to look at different aspect of cognition. During that time, and during that work, I realized that something very important was missing in our equation of understanding the development of individuals and people with Down syndrome: and that missing piece was sleep.
This realization pushed me to go and look elsewhere. I was very lucky: there was a group at the University of Arizona that had just started a very interesting study looking at the relationship between obstructive sleep apnoea and different cognitive outcomes in children with Down syndrome. I took the this opportunity, flew to the University of Arizona, and joined their group. Since then, we have been looking at different aspects of sleep in children with Down syndrome across their lifespan in relation to different aspects of life, quality of life, and behaviour.
We now know that sleep isn't just a time where the brain rest. We actually take care of all the things that we cannot do while we're awake. This is very important when we think about neurodevelopmental conditions like Down syndrome, because during this period, we actually put together all the information that we learn during the day. We integrate new information. If you don't sleep well, as is the case for children with Down syndrome, this integration doesn't happen. This is what we found in a previous study, in terms of memory consolidation in children with Down syndrome, who were not using the sleep interval to remember in the same way as their neurotypical peers. This means that even the best educational and behavioural interventions might not be as effective as they can be, if we do not address sleep problems in this population.
Addressing sleep isn't just about getting a good night’s sleep. It's about supporting learning, development, and well-being in this population. That's why I'm very proud of to be part of the Down Syndrome Sleep Research Network, where we come together, (researcher, clinician, and different people) to share knowledge, advance research - and ultimately, the goal is improving sleep and other outcomes in people with Down syndrome. Thank you!
You can find out more about Dr Spano’s academic work at this link.
Launch Event for the Down Syndrome and Sleep Research Network - London, 9th June 2025
The DSSRN was launched earlier this year with keynote speakers across many different research areas. We are excited to see the new developments that will come from so much skill and dedication focused on tackling challenges with sleep in the Down syndrome community.
Watch the overview of the launch day to see what we covered, and signposts of where we’ll go from here.
Short interviews with some of the speakers and attendees at the launch can be seen at our YouTube playlist about Down Syndrome and Sleep Research.
Sleep Webinar Part 1: Dr Liz Corcoran - Why focus on research about sleep and Down syndrome?

Edited transcript of YouTube video.
It is lovely to have you all here for this webinar about sleep, and the particular issues our loved ones with Down’s Syndrome might face in the night time hours, or at other times.
I want to take a moment to tell you a little about who we are, as an introduction, in case you have never heard of us. The Down’s Syndrome Research Foundation has been around for over 20 years.
I am Dr Liz Corcoran, I am a sibling to David, who has Down’s syndrome. He is the adult you see in some of the photos here, and he has kindly shared his pictures from his sleep study a little while ago. He was very happy to share with people, particularly with younger people who have to face doing a sleep study as well: just to show them that it wasn’t scary at all. Actually, he has been managing to wear his CPAP machine every night - most nights!
That’s why I am involved with Down’s syndrome and the Down’s Syndrome Research Foundation. We are the UK's only Down’s syndrome research charity and our vision is for people with Down’s syndrome to have a long, healthy, and happy life. We know also that families are impacted as well.
We want to bring you the best scientific research needed for the issues that affect our community. We do this by funding and promoting groundbreaking research, as we want to improve understanding of Down’s syndrome. A further important part of what we do is supporting the human rights of people with Down’s syndrome and their families, through advocacy. You may have heard of some of our recent victories. We're very happy about the restarting of the Down’s syndrome APPG (All Party Parliamentary Group) and the Down’s syndrome Bill that's being proposed and moving through Parliament. We’re very happy to be a small part of the work that's going on there, behind the scenes.
Why does research matter? It has important impacts. First, it means that people with Down’s syndrome can get evidence-based treatment. There are lots of questions – particularly holes in research around sleep. However, there are also lots of other places where we lack good guidance and good evidence on the best treatments for people with Down’s syndrome, when they have particular conditions or problems. We want them to live richer lives, to have the best quality of life, and to have healthier lives.
I often talk to local groups, about nutrition, and about lifestyle: sleep is a huge part of that. As a foundation we want to support sleep research and promote understanding of good sleep.
We also do advocacy work because we want people with Down’s syndrome to have choices and to be able to live the life they would want to live.
That includes helping to make sure there's up-to-date research, and that they have equal rights to research funding. At the moment, you may not be aware that just over five pounds per person with Down syndrome per year is spent on research. We think this is terrible, and we'd like to see that number change. We need to lobby the government to improve this, but we also need to mobilize the community, to understand why research matters.
This is just one aspect. I want to spend a little bit of time inspiring you, particularly that this is just one aspect, sleep that impacts people with Down’s syndrome.
If I can encourage you to get behind the work of the Foundation and support research in any way you can, we would be so grateful.
This segment is part of a full length Webinar.
Down Syndrome and World Alzheimer’s Awareness Month
September is World Alzheimer’s Month – dedicated to raising awareness of a condition which is increasingly affecting the general population. This condition is particularly relevant to the Down syndrome community, where prevalence is much higher than average. To help increase awareness, we have gathered some resources and recent news that is important to know about both Down syndrome and Alzheimer's, and some helpful directions to look for more advice and practical help.
The Alzheimer Biomarkers Consortium-Down Syndrome (ABC-DS) says: “Did you know that 70% of adults with Down syndrome will develop Alzheimer’s at some point in their life? Virtually all people with Down syndrome have brain changes consistent with Alzheimer’s by age 40. This needs to change. The only way to change these odds is to better understand, diagnose, treat, and prevent Alzheimer’s in the Down syndrome community.”
Alzheimer’s and the Down Syndrome and Sleep Research Network (DSSRN)
There is an important but under-researched link between sleep quality and the onset of dementia. Researchers involved in DSRF UK’s newly launched Down Syndrome and Sleep Research Network (DSSRN) are keen to explore these connections in relation to Down syndrome. Improving sleep has the potential to decrease the risk of dementia in people with Down syndrome.
Dr Stephanie S. G. Brown Ph.D. is Senior Research Associate and Alzheimer's Research UK Fellow in the Department of Psychiatry at the University of Cambridge. At the launch of the DSSRN, she presented new research focused on the development of dementia in Down syndrome, investigating sleep as a mediating factor in the onset of Alzheimer's disease. You can sign up for the excellent ‘Defeating Dementia in Down Syndrome’ newsletter by emailing: CIDDRG@medschl.cam.ac.uk
We are eager to help build on research like this, to pioneer interventions and treatments that will improve brain health.
News on Alzheimer’s and Down Syndrome Research
It is becoming more evident that it is greatly worthwhile to invest in research on Down syndrome and Alzheimer’s. A few recent news articles have shown new leads in treatment possibilities, including an article in July 2025 exploring the possibility of using sleeping pills to reduce protein buildup that causes Alzheimer’s, and another article in August 2025 which identifies that women with Down syndrome are more at risk of developing Alzheimer’s than men. The article points out: “This insight points to the need for more sex-specific approaches in both Alzheimer’s research and treatment planning, especially in the design of clinical trials.”
Practical Action and Further Information
DSRF UK will soon be starting up a new public education blog on the DSSRN website, with information on sleep research and DS, including current research on the connections between quality of sleep and onset of dementia.
We are also planning to offer practical workshops for parents and carers via the DSSRN, on how to improve brain health through improved sleep. More information will be forthcoming as plans develop.
Researchers have been briefing the All-Party Parliamentary Group on Down Syndrome (APPGDS) with information specific to DS and Alzheimer’s, to bring awareness of this issue directly to the UK government and highlight the need for funding to be dedicated to this area.
It is also our hope that the upcoming Guidance on the Down Syndrome Act, due to be issued soon, will specifically take into account the need for improved health services related to tackling Alzheimer’s for people with Down syndrome.

Adaptability of sleep and the ‘sleep privilege’: the need for new research
How much should parents and caregivers worry about sub-optimal sleep? This issue was recently brought to our attention by Professor Alice M Gregory, a keynote speaker at the recently launched Down Syndrome and Sleep Research Network (DSSRN).
Sleep issues are over-represented and under-researched in the Down syndrome community. This gap is a driving motive for the DSSRN, and through this new research network, we hope to accelerate knowledge and effective interventions in this area.
The effect of broken sleep often weighs on parents and carers. This includes the health impact of poor sleep on family members with Down syndrome, but also the consequences of long-term interrupted sleep on caregivers themselves.
Prof Gregory has been involved in research with particular interest for caregivers. Her presentation at the DSSRN launch, “Type 1 diabetes as a prototypical condition challenging what we know about sleep”, opened up very interesting considerations about the pitfalls of an exaggerated focus and concern about quantifying and qualifying sleep.
Sleep is certainly more important for health and development than we have realised historically, but there are adaptive patterns that are even less understood, which may help compensate for some quantifiable sleep deficits.
This ability to adapt is also an under-researched area. Exploring this further will bring solid evidence that can help shape practice and guidance. This may be very good news for many people who simply cannot secure the ‘sleep privileges’ that others enjoy, and may ease some of the worries that come along with poor sleep.
We believe that this topic is just one of many areas that will benefit from the support of the DSSRN, bringing researchers together to change what we know about sleep in the DS community.
For further details on this topic, you can read a newly published editorial in the Journal for Child Psychology and Psychiatry, by Professor Alice Gregory et al, “Sleep privilege – research and clinical recommendations for when sleep cannot be optimal”.

World’s first research network focused on sleep issues and Down syndrome launched 9th June 2025
Researchers from institutions across the UK gathered in London to foster cooperation in tackling sleep disorders that can profoundly affect health and development in the Down syndrome community.
The Down Syndrome and Sleep Research Network (DSSRN) was officially launched on Monday at the conference hall of the National Council for Voluntary Organisations, as an initiative to bring scientists together to concentrate on one of the highest priorities and most promising focal points for improving quality of life for people with Trisomy 21.
Sleep issues are common in people with DS, being detected up to ten times more than in typically developing peers. Researchers are keen to explore how improvements in sleep could positively impact development, cognition, chronic illnesses, and also longevity in a population whose life expectancy is at least 20 years lower than average.
Presenters included academics and researchers from University of Cambridge, Kingston University, Royal Holloway, Great Ormond Street and other institutions, presenting on their individual work and setbacks they have faced as researchers. A panel discussion with five interdisciplinary researchers generated a lively conversation on the challenges and opportunities in this area.
Keynote speaker Dr Lizzie Hill (Senior Lecturer in Sleep Physiology, University of the West of England (UWE Bristol) said “All of us in this room have heard something to the effect that ‘people with Down syndrome don’t sleep well’ or 'it's just part of the condition', but that doesn't mean we shouldn't investigate and treat these as we would for anyone else.”
A poll of attendees on the day showed that 55% of attendees were currently involved in research, and 45% planning / would like to get involved, but experiencing barriers including lack of funding, lack of time and high workload, lack of research skills and knowledge, lack of support, bureaucracy and admin issues, ethics and regulatory processes, difficulty finding collaborators. Many of these issues were addressed on the day to explore ways forward.
The DSSRN has secured funding for its startup year with generous grants from Hospital Saturday Fund, the Baily Thomas Charitable Trust, and the Sir Samuel Scott of Yews Trust, and the Launch Event was sponsored by Inspire Medical Systems and Idorsia. The DSSRN’s founding and launch have been coordinated by the Down Syndrome Research Foundation UK (DSRF UK), a charity promoting and funding medical research to improve the lives of people with Down syndrome since 1996.
DSRF UK’s Chair Dr. Elizabeth Corcoran said: “It has been a dream to bring these highly renowned researchers together to begin pooling their knowledge and expertise. We have great hope that with their combined insights, we’ll see breakthroughs in science in this area. This will yield new treatments that will give people with Down syndrome better sleep, from early childhood to adulthood, which will be a foundation for much healthier and longer lives.”
If you wish to stay in contact for updates, please fill out the form here: https://dssrn.org.uk/contact
Queries for the Down Syndrome and Sleep Research Network can be directed to: info@dssrn.org.uk